Quick Facts
- Threshold: Dialysis typically begins when your Glomerular Filtration Rate drops below 15 mL/min/1.73m², signaling Stage 5 CKD.
- Preparation: A surgical Arteriovenous fistula requires approximately 3 months of maturation time before it can be used for treatment.
- Adequacy: To ensure your blood is being cleaned properly, the target Kt/V ratio is 1.2 for clinic-based hemodialysis and 1.7 for peritoneal dialysis.
- Heart Health: Peritoneal dialysis may offer clinical advantages for patients with congestive heart failure due to its gradual fluid removal process.
- Nutrition: Maintaining high-quality nutrition is vital, with a serum albumin goal typically set above 4.0 g/dL.
- Global Context: As of 2023, roughly 4.6 million people globally were receiving kidney replacement therapy.
Navigating a diagnosis of End-Stage Renal Disease (ESRD) can be overwhelming. This dialysis treatment guide is designed to decode your options, from understanding clinical thresholds like Glomerular Filtration Rate to choosing between hemodialysis and peritoneal dialysis. As of March 2025, there were 516,837 patients undergoing dialysis in the United States. Whether you are planning the transition to kidney replacement therapy or seeking to improve your current care, understanding the metrics of dialysis adequacy and the preparation required for vascular access is essential for long-term health and vitality.
Choosing between hemodialysis and peritoneal dialysis involves comparing lifestyle needs and clinical factors. Hemodialysis typically occurs thrice weekly in a clinic, focusing on rapid waste removal, while peritoneal dialysis is a daily home-based therapy using the abdominal lining as a filter. For patients with congestive heart failure, peritoneal dialysis may offer hemodynamic advantages through gradual ultrafiltration, potentially reducing cardiac strain compared to the rapid fluid shifts in hemodialysis.
Recognizing the Threshold: When to Start Dialysis
The transition from Stage 4 to Stage 5 Chronic Kidney Disease is a pivotal moment in your health journey. For most patients, the clinical indicator to begin therapy is when the Glomerular Filtration Rate falls below 15. However, this number is only one part of the equation. Your care team will also look for physiological triggers such as persistent fluid overload, which can strain the heart, or hyperkalemia, a dangerous buildup of potassium.
Learning how to monitor dialysis adequacy through medical metrics starts even before your first session. Many adults remain unaware they have kidney disease until it reaches an advanced stage. Once diagnosed with ESRD, the focus shifts toward total electrolyte management. Your nephrologist will track your lab results closely to determine the precise moment your kidneys can no longer maintain a safe internal environment. This proactive monitoring helps prevent emergency starts, which often carry higher risks of complications.
Comparing Modalities: Hemodialysis vs. Peritoneal Dialysis
Choosing your path requires a deep dive into the types of dialysis compared by both clinical efficacy and daily lifestyle impact. This hemodialysis and peritoneal dialysis guide highlights that while both therapies save lives, they do so in very different ways.
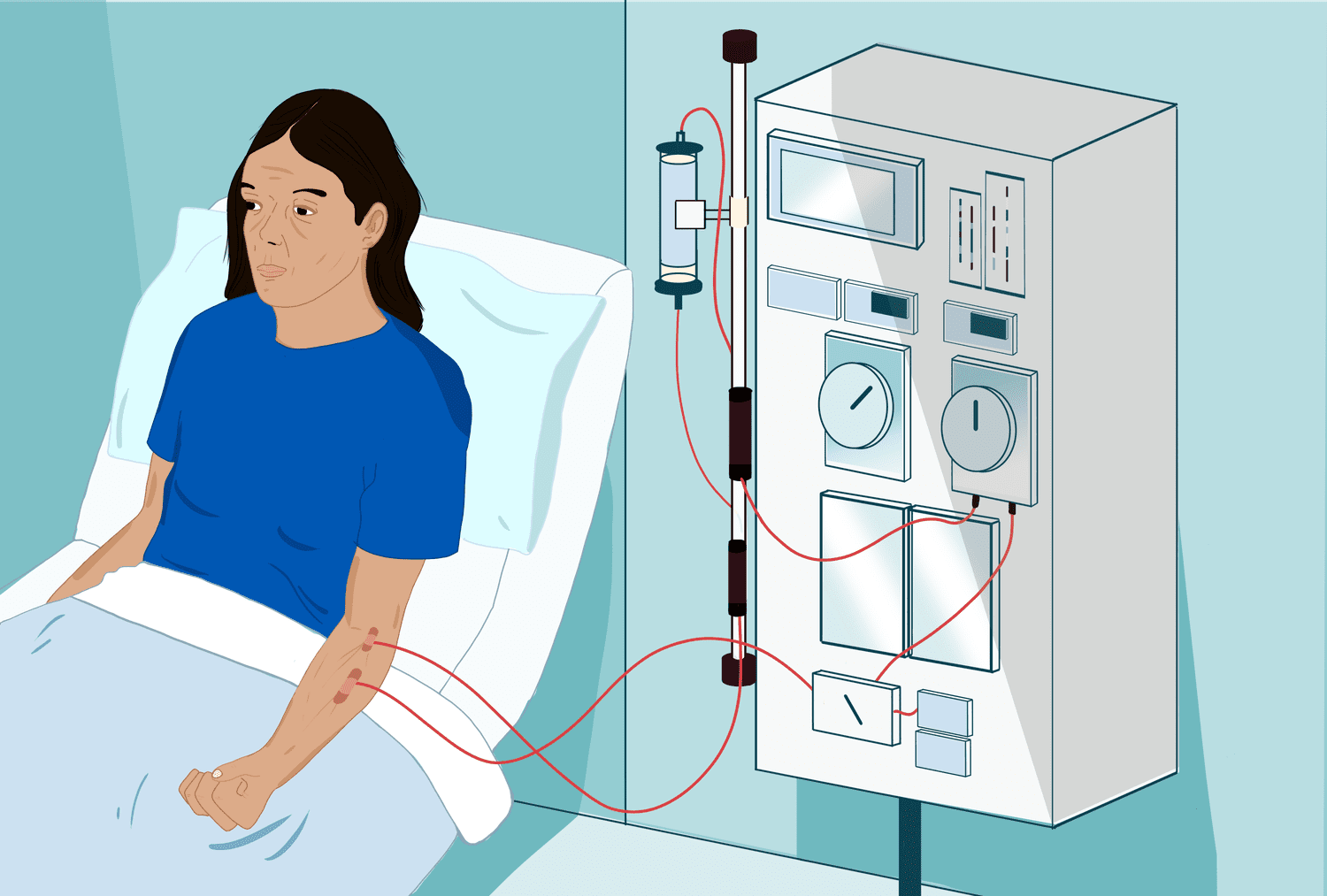
Hemodialysis is the most common approach. It generally involves traveling to a specialized center for three sessions per week. During these understanding the requirements for thrice weekly hemodialysis sessions, your blood is pumped through an external filter called a dialyzer. This method uses hydrostatic pressure to quickly strip away toxins and excess fluid. However, this rapid shift can sometimes lead to intradialytic hypotension, where blood pressure drops suddenly during the treatment.
In contrast, peritoneal dialysis offers a more flexible, home-based alternative. It uses the lining of your own abdomen—the peritoneum—as a natural filter. A sterile dialysate solution is introduced into the abdominal cavity via a permanent catheter. This process happens daily, often while you sleep, using a machine called a cycler. For those choosing between hemodialysis and peritoneal dialysis for home treatment, the daily nature of peritoneal dialysis mimics natural kidney function more closely than intermittent clinic visits.
There are also specific dialysis treatment considerations for patients with congestive heart failure. Because peritoneal dialysis removes fluid slowly and continuously over 24 hours, it places significantly less stress on the heart. Clinical data suggests this gradual ultrafiltration can help maintain hemodynamic stability, making it a preferred option for those with pre-existing cardiac issues.
Preparation and Vascular Access: The 3-Month Window
One of the most critical steps in your dialysis treatment guide is the preparation of your vascular access. This is the "lifeline" through which your blood is cleaned. If you choose hemodialysis, the gold standard is an Arteriovenous fistula. This is a surgical connection between an artery and a vein, usually in your arm.
The catch is that an Arteriovenous fistula requires time—typically three months—to "mature" and become strong enough for regular use. Patients who wait until the last minute often have to rely on a central venous catheter, which carries a much higher risk of infection and blood clots. Planning ahead and ensuring proper vascular access care is one of the best things you can do to ensure long-term success. If you opt for peritoneal dialysis, you will instead require a small surgery to place a catheter in your abdomen, which generally requires about two weeks of healing before it can be used.
Navigating Daily Life and Monitoring Quality Metrics
Living with end-stage renal disease requires a shift in how you view your daily health. It isn't just about the time spent on a machine; it is about the constant management of your body’s chemistry. A key part of this is managing hemoglobin levels and anemia in dialysis patients. Because the kidneys produce a hormone called erythropoietin that tells the body to make red blood cells, most ESRD patients require Erythropoiesis-stimulating agents to prevent severe fatigue and weakness.
To ensure your treatments are effective, your team will use specific quality markers. The Kt/V adequacy ratio and the Urea reduction ratio are the primary tools used to measure how well urea is being cleared from your blood. If these numbers are too low, it means you aren't getting enough dialysis, which can lead to a buildup of toxins and a decrease in your overall well-being.
| Metric | Target Goal | Clinical Importance |
|---|---|---|
| Kt/V (Hemodialysis) | 1.2 or higher | Measures the volume of fluid cleared of urea. |
| Kt/V (Peritoneal) | 1.7 or higher | Ensures daily waste removal is sufficient. |
| Urea Reduction Ratio (URR) | 65% or higher | Measures the percentage of urea removed per session. |
| Serum Albumin | > 4.0 g/dL | Indicates nutritional status and protein intake. |
| Hemoglobin | 10.0 - 11.0 g/dL | Prevents anemia-related heart strain and fatigue. |
Beyond the lab, practical daily life management for end-stage renal disease involves strict fluid restrictions. Since your kidneys can no longer process excess water, drinking too much between sessions can cause swelling and high blood pressure. You will also work closely with a renal nutritionist to manage your intake of potassium, sodium, and phosphorus. Most patients take phosphorus binders with every meal to prevent this mineral from leaching calcium from their bones.

Building Your Interprofessional Care Team
Success in treating ESRD is a team sport. Your primary contact is the nephrologist, but your renal nutritionist and social worker are equally important. They help you navigate the complex emotional and physical changes that come with kidney failure. You should also utilize the CMS Quality Reporting System to evaluate different facilities. This system tracks how well centers meet targets for hemoglobin and urea reduction, giving you the data needed to choose the safest environment.
Among Americans newly diagnosed with kidney failure in 2022, nearly 97% began life-sustaining dialysis treatment, while only a small fraction were able to receive a preemptive transplant. It is vital to discuss transplant eligibility early in your journey. Even if you start on dialysis, being on the waitlist or finding a living donor can change your long-term outlook. Your care team will track your residual renal function—the small amount of kidney function you may still have—to adjust your dialysis prescription and keep you as healthy as possible for a future transplant.
FAQ
What are the different types of dialysis treatment?
The two main categories are hemodialysis and peritoneal dialysis. Hemodialysis uses a machine and a special filter called an artificial kidney to clean your blood. Peritoneal dialysis uses the lining of your abdomen and a cleaning solution to remove waste. Hemodialysis can be done in a center or at home, while peritoneal dialysis is almost always done at home.
What is the difference between hemodialysis and peritoneal dialysis?
The primary difference is the method of filtration. Hemodialysis filters blood outside the body using a machine and typically happens three times a week for several hours. Peritoneal dialysis uses the body's peritoneal membrane as the filter and is a continuous, daily process. Hemodialysis often involves more rapid fluid removal, while peritoneal dialysis is more gradual.
Can you perform dialysis at home?
Yes, both hemodialysis and peritoneal dialysis can be performed at home. Home hemodialysis usually requires a partner and more intensive training, while peritoneal dialysis is designed specifically for independent home use. Home therapies offer more flexibility with scheduling and often lead to better overall health outcomes due to more frequent treatments.
How long does a typical dialysis session take?
In-center hemodialysis usually takes about 4 hours, performed three times a week. Home hemodialysis sessions may be shorter but more frequent, such as 2 to 3 hours five days a week. Peritoneal dialysis is typically performed every day; if using a cycler machine, it usually happens during 8 to 10 hours of sleep.
What should you eat while undergoing dialysis treatment?
A renal diet focuses on high-quality protein while limiting sodium, potassium, and phosphorus. You will need to carefully monitor fluid intake to prevent swelling and heart strain. Most patients work with a renal nutritionist to create a meal plan that balances these needs while ensuring enough calories to maintain strength.
How long can a person live on dialysis?
Life expectancy on dialysis varies greatly based on age, underlying health conditions, and how well the treatment plan is followed. Many people live for 5, 10, or even 20 years or more on dialysis. While it is a life-sustaining therapy, for many, the ultimate goal is to remain healthy enough to qualify for a kidney transplant.


